Über den Autor

Dr. Omar Soliman
South Valley UniversityQena - Nqada
83523 Qena Governorate, Egypt
Germany
Dr.omar.soliman@outlook.de
http://www.svu.edu.eg
A comparative clinical study between crestal incision approach and kazanjian vestibuloplasty during ridge augmentation for an atrophied posterior mandible using bone block
Thema
Reconstruction of an atrophied posterior mandible is challenging because the deformity involves deficiency in both the bone and the mucosa (Oda T et al., 2002). Managing a patient with an atrophied posterior mandible is complicated, as we have to overcome various complications in order to have him properly rehabilitated, such as:
- A surgical problem when placing the implant, due to insufficient bone quantity above the inferior alveolar nerve.
- A prosthetic problem, due to an increase inter arch space, which lead to an improper crown-root ratio.
- An anatomic problem, since the mandible is not like maxillary sinuses, which provide a natural cavity for containing grafting material, retain it in its place without movement, good soft tissue cover without tension protecting the graft material from infections (Chaushu et al., 2009). Thus, the graft, which is used in the reconstruction of an atrophied posterior mandible, must have sufficient strength and rigidity to fixate at the recipient site through three-dimensional stability in order to withstand muscular forces (Moy & Palacci, 2001), which possibly move the graft buccolingually.
- Soft tissue management is very complex during the reconstruction of a posterior mandible. Critical elements must be taken into consideration when planning the treatment. The reason why incision line opening is more common during bone grafting is because the overlying tissue must be advanced over a larger volume of bone and the tension on the incision line may pull the soft tissue apart. A Good flap designed in the way that you place the graft with a tension-free flap is necessary for achieving successful bone regeneration and long-term peri-implant tissue stability. Soft tissue coverage is a prerequisite for successful bone augmentation and a lack of soft tissue, on the other hand, may prevent bone gain. In such situations it might be advisable to first augment the volume of the soft tissues and then perform the bone augmentation procedure as a second step.
Objective
The aim of this study was to evaluate and compare the clinical outcomes of bone block ridge augmentation using two flap design approaches (crestal incision and Kazanjian vestibuloplasty).
Materials and Methods
A. Subject selection
20 patients were included in this study. All of them needed bone-block augmentation procedures because of severe alveolar ridge atrophy in the posterior mandible. The patients were randomly divided into two groups with 10 patients each: the first group (group A) was scheduled for ridge augmentation by using the crestal incision approach and the second group (group B) was scheduled for ridge augmentation by using Kazanjian vestibuloplasty. In both groups NanoBone blocks were used.
B. Ridge augmentation procedures
Under local anaesthesia, Kazanjian vestibuloplasty was done according to the methods described by Khoury et al., 2007. A horizontal incision was made far from the vestibule, dissecting the epithelial barrier and the submucosa. After preparing a supra-muscular partial-thickness flap in the direction of the alveolar crest, the periosteum is cut at the mucogingival junction and a full-thickness flap is prepared in the lingual site. Using a scalpel, the muscle attachment towards the buccal periosteum is dissected and the muscles are detached in apical direction. After augmentation, the buccal periosteum was resutured to the lingual part and, in a second step, the split-thickness flap is sutured in the vestibule to the buccal periosteum to prevent relapse of the muscle attachment (Khoury et al., 2007). The horizontal incision made in the mucosa of the vestibule must be related to the volume of the bone that is about to be grafted, so that the partial-thickness flap is large enough to cover the graft at the end of surgery. After dissection of the muscle in apical direction, the periosteal flap is decollated from the underlying bone, exposing the thin crest. After bone augmentation, the buccal periosteum is resutured to the lingual flap, covering the grafted area as a first layer of closure. The partial-thickness and lingual pediculated flap is then reflected back and sutured to the periosteum as far as possible in the vestibule to prevent the muscle attachment from relapsing, representing a second layer of closure over the grafted area.
Crestal incisio
A full-thickness crestal incision was made and the soft tissues overlying the reconstructed alveolar process were elevated (Felice et. al., 2009).
Bone block fixation
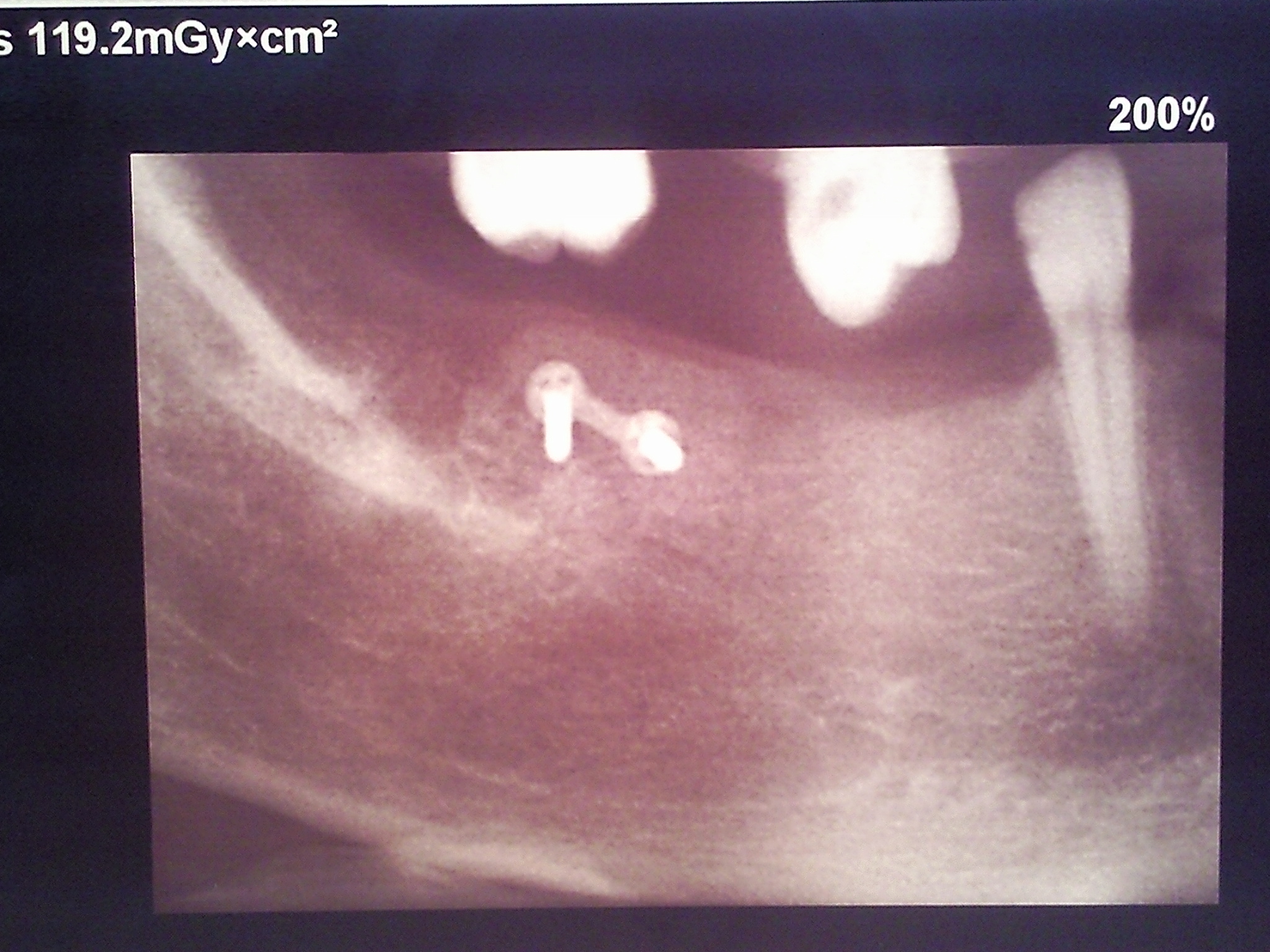
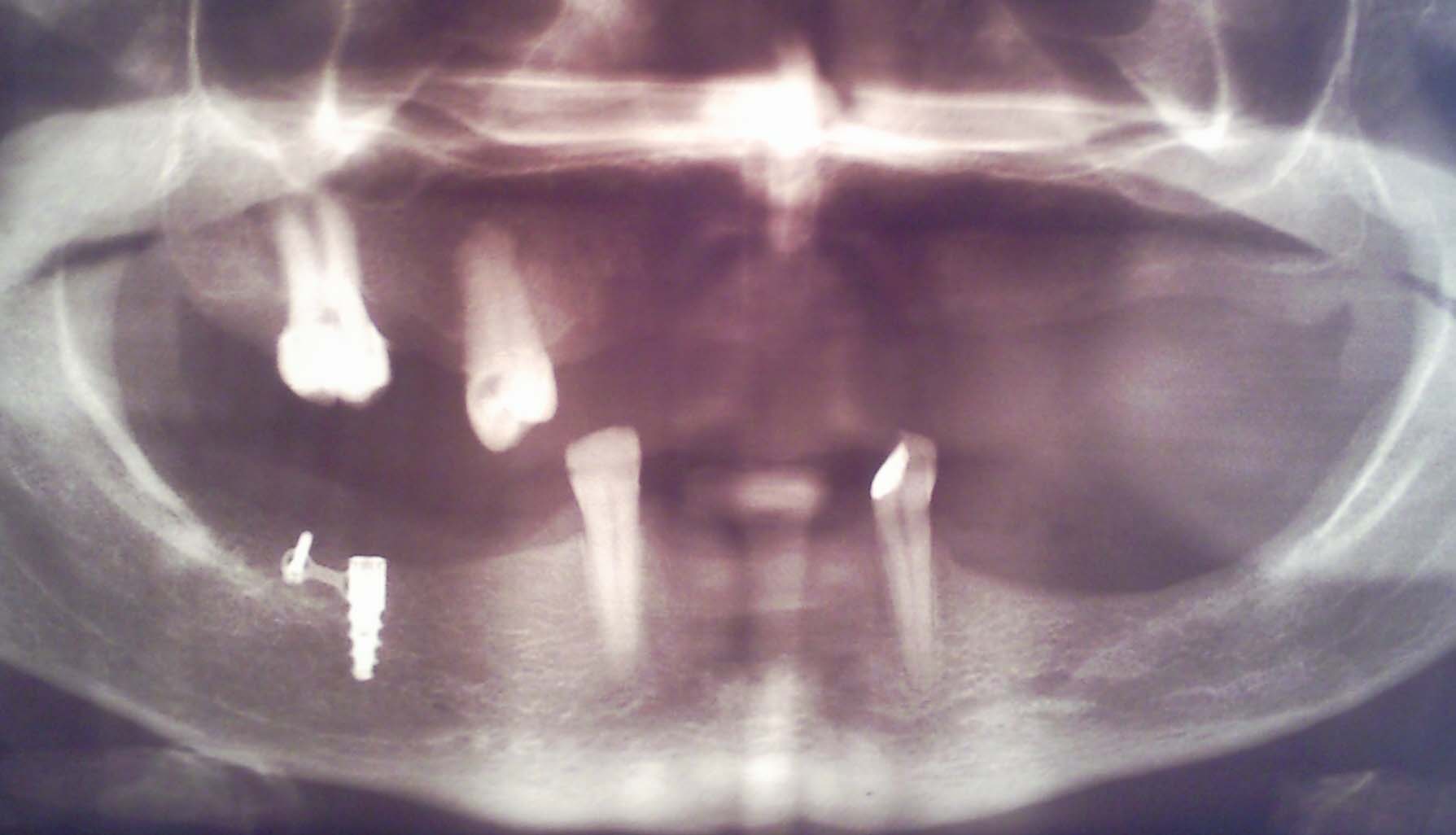
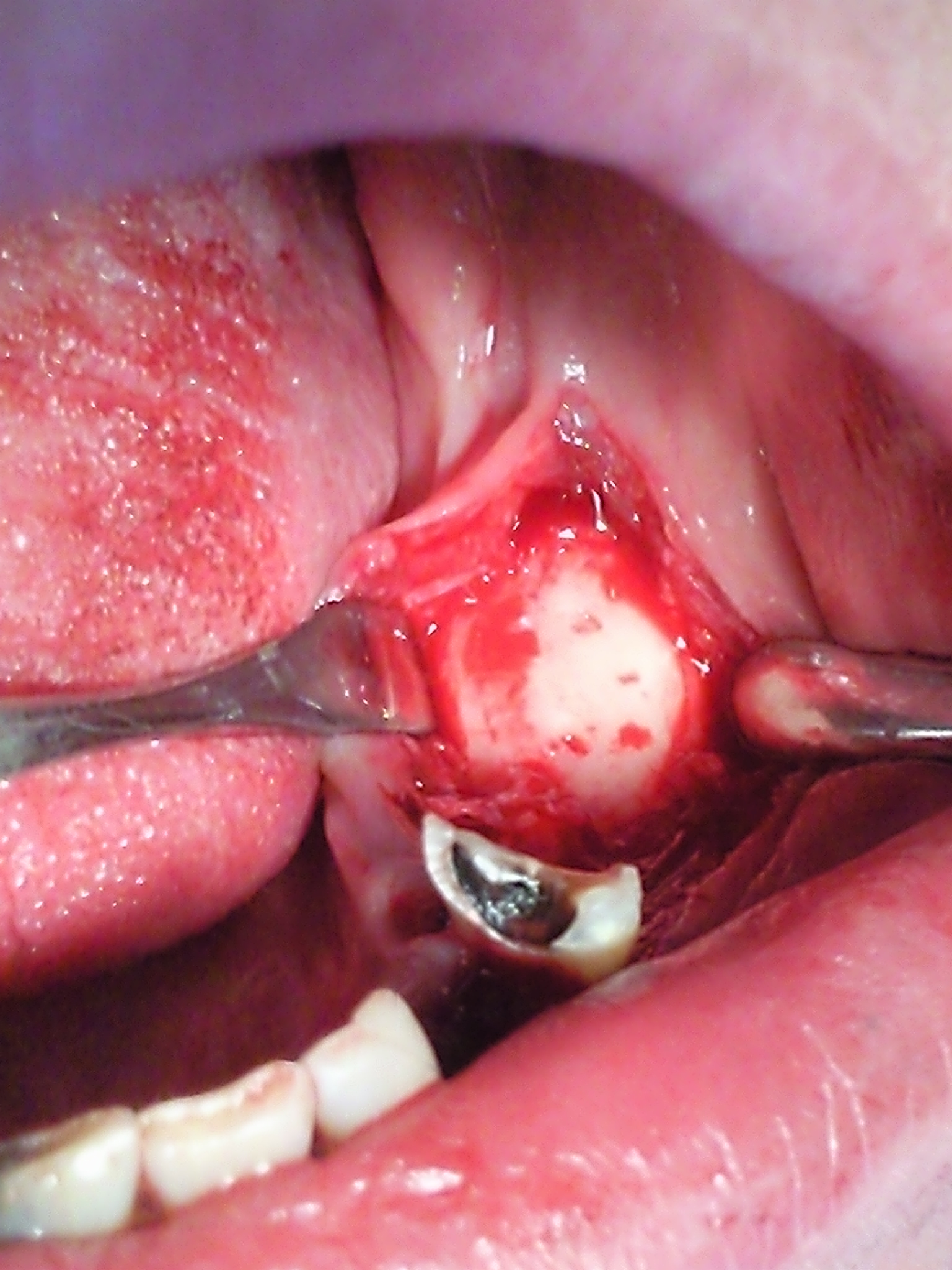
After exposure of the bone surface, some bleeding points were created using a fine round bur through the vestibular corticalis (Merten and Steveling, 2009). The bone block was adapted to the ridge using a scalpel. When the blocks lie flush against the ridge, they were fixed with a 2-hole microplate and two microscrews. Thereafter, the edges were smoothed. After bone augmentation, the buccal periosteum was sutured to the lingual part, covering the grafted area as first layer of exposure. The partial thickness and lingual pediculated flap was reflected back and sutured to the periosteum as far as possible in the vestibule, to prevent relapse of the muscles attachment, representing a second layer closure over the grafted area (Fig. VI-9) (Khoury et al., 2007).
Results
Group A (Kazanjian vestibuloplasty): No intra-operative complications were present during the augmentation procedures. In addition, no post-operative complications were present after the ridge augmentation or at the time of the implant surgery, except for one case of infection.
Group B (crestal incision): During intra-operative procedures, NanoBone augmentation was associated with fracture of the NanoBone block during augmentation in one case, because it was fragile and fractured easily. In the post-operative period, soft-tissue complications such as the incision line opening, a small perforation of the mucosa over the grafted bone, and graft infection occurred. In addition to partial graft exposure, screw exposure and screw loss, one block graft was completely exposed (30 days after surgery) and lost.
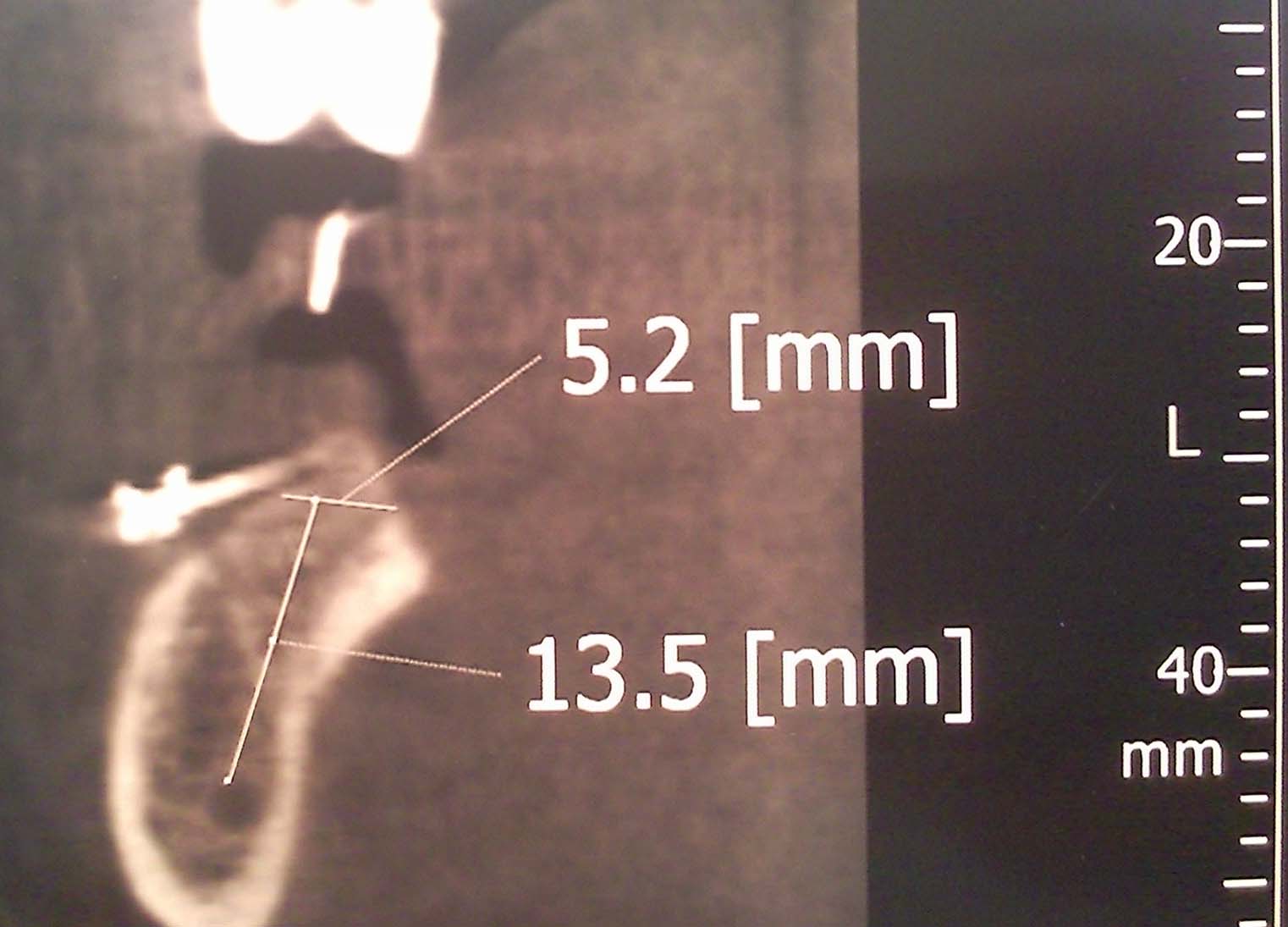
Both groups: The regenerated ridges healed uneventfully and no evidence of serious adverse local reactions, i.e. foreign-body reaction, pain, dysaesthesia, inflammation was observed in any patient throughout the study. By comparing CBCT scans before and six months after the augmentation procedures, it was found that CBCT is not a suitable means of evaluation for ridge augmentation with either NanoBone blocks. It was surprising that NanoBone density was greater after grafting. This was because of the presence of mineral in NanoBone, which acts as a scaffold that degrades progressively and is replaced by new bone eventually. The new bone is premature with a low mineral density and therefore not radiopaque after six months to seen as radiopaque.
Discussion
Primary soft tissue closure is a mandatory precondition for the success of grafting procedures. It ensures healing by primary intention and requires minimal soft tissue existence, rapid collagen formation and soft tissue remodelling. It also minimises postoperative discomfort for the patient. It is a necessary step for achieving predictable bone regeneration. The opening of the incision line during initial healing is the most common postoperative complication in intra-oral bone grafting (Schwartz-Arad D et al. 2005). As a result, the graft is contaminated or lost and bone growth is impaired (Locci P et.al.1997).
The reason of incision line opening is more common during bone block grafting because the overlying tissue must be advanced over a larger volume of bone and the tension on the incision line may pull the soft tissue apart. In addition, the soft tissues are poor in local growth factors under the reflected flaps that lie over a graft material or barrier membrane, rather than the host bone (Misch et al., 2008).
Dehiscence and flap necrosis: These soft-tissue complications are frequently the result of vascular compromise caused by inadequate planning, insufficient flap range or excessive surgical trauma, especially in smoking patients. Also, mechanical over- loading of the grafted area with a removable prosthesis or through biting of the antagonist teeth could also be the cause of complication, with exposure of the graft to the complex microbiological spectrum in the mouth and graft infection which leads to graft degradation and total failure of the procedures. Dehiscence may occur because of premature separation of sutures as a result of inadequate suturing or tensions on the soft tissues. Retraction of a soft tissue flap is most likely where the vestibule is shallow or the muscle pull is great.
Exposure of the screws: During the healing process, a decrease in graft volume is a normal sign of the remodelling process. Vorhoeven et al. 2000 reported a loss of up to 25% of the overall height of bone graft. While the bone volume decreases, the fixation screws stay in their original position and may emerge through the overlaying soft tissue. In the early stages of the healing, the screws have to stay in place for proper stabilisation of the graft. In the later stage, exposed screw can be removed. The soft tissue perforation will heal properly after a couple of days.
Exposure of part of the graft: Knife-edge graft can provoke perforation of the overlying soft tissue with subsequent dehiscence. In addition, pressure from a removable temporary prosthesis can create local irritation and dehiscence, which will jeopardise the success of the operation. Hollowing out of existing provisional prosthesis to avoid direct contact with the wound bed is another key factor for success in bone graft procedures.
If a small dehiscence occurs after block grafting, treating the site with chlorhexidine gel and mouth rinse can be attempted until wound closure. Exposed bone chips have to be removed. Exposed parts of the graft are considered to be contaminated and debridement with a bur has to be performed. Surgical intervention is used to achieve soft tissue closure only when the early stage of soft tissue healing is over. After the initial healing process, debridement of the graft has to be performed and a conventional flap design may be used to try to close the soft tissue. If the site is not covered with soft tissue during the first two weeks after intervention, the complete graft has to be removed.
Bildergalerie (22)


















Literatur:
- Chaushu, G.; Mardinger, O.; Calderon, S., Moses, O.; Nissan, J: The use of cancellous block-allograft for sinus floor augmentation with simultaneous implant placement in the posterior atrophic maxilla. Journal of Periodontology 80: 422-428, 2009.
- Felice P, Lezzi G, Lizio G, Pittelli A, et al.: Reconstruction of atrophied posterior mandible with inlay technique and mandibular ramus block graft for implant prosthetic rehabilitation. Int J Oral Maxillofac Surg 67:372-380, 2009.
- Khoury F and Happe A: Soft tissue management in oral implantology. A review of surgical techniques for shaping an esthetic and functional pre-implant soft tissue structure. Quintessence Int , 31:483-99, 2000.
- Khoury F et al.: Bone augmentation in oral implantology. Quintessence publishing Co. Ltd. Page 81-84, 2007.
- Locci P, Calvitti M, Belcastro S et al.: Phenotype expression of gingival fibroblasts cultured on membranes used in guided tissue regeneration, J Periodontol 68:857-863, 1997.
- Merten C and Steveling HG: Use of Synthetic Bone Blocks as an Alternative to autologous Bone Blocks Grafts. A case report. Implants 4:30-33, 2009.
- Misch CE: Diagnostic imaging techniques. Misch CE, editor. Contemporary Implant Dentistry, 3rd ed. St Louis: CV Mosby Company; p. 38-67, 2008.
- Moy, P. and Palacci, P: Minor bone augmentation procedures, soft and hard tissue management. Esthetic implant dentistry 23:137, 2001.
- Oda T, Sawaki Y, Ueda M: Alveolar ridge augmentation by distraction osteogenesis using titanium implants: An experimental study. Int J Oral Maxillofac Impl;17:52, 2002.
- Schwartz-Arad D, Levin L and Sigal L: Surgical success of intraoral autogenous block onlay bone grafting for alveolar ridge augmentation, Implant Dent 14:131-138, 2005.
Zusammenfassung:
Kazanjian vestibuloplasty is better than crystal incision as an approach for bone block ridge augmentation in atrophied posterior mandibles. The reasons are:
- It provides adequate space for containing the bone block and for suturing the flap without tension. This space is proportional with the bar tissue left in buccal mucosa.
- It completely covers the graft and the incision line is away from the graft, which protects the graft from the infection.
- Unlike crystal incision flap, the lingual flap is not completely dissected from the inner aspect of the mandible, and maintain the vestibule. This decrease muscle tension preventing the movement on both sides of the wound preventing, the appearance of wound dehiscence and incision line opening. These are not rare complications after crestal incision, due to muscle tension, which may compromise the prognosis of the underlying grafted bone.
- The reason of incision line opening is more common in crystal incision bone block grafting because the overlying tissue must be advanced over a larger volume of bone and the tension on the incision line might pull the soft tissue apart. In addition, the soft tissues are poor in local growth factors under the reflected flaps that lie over a graft material or barrier membrane, rather than the host bone (Misch et al., 2008).
Recommendation
Kazanjian vestibuloplasty should be modified by performing only vestibular and mesial vertical incision and not performing distal vertical incision, because distal vertical incision prevents blood flow from posterior area to the flap. By doing that, blood flow to flap will be from lingual side supplied by the sublingual artery and posterior area supplied by the facial artery and muscular branches of the maxillary artery.